Sunday, September 4, 2011
An Update
As of right now, I have been cancer free for close to 13 months. I'm back at Yale for my senior year after having worked for 6 months, first at a Palo Alto software company and then at a finance firm in New York. I'm certainly not in the best shape of my life, but my health is no longer an all consuming problem. I'm incredibly grateful that it has recovered to the point where I could work at those two companies, both of which are on this list. Indeed, the other day I caught myself saying "I've had a good year" which I had to quickly amend to "I've had a good six months."
Friday, May 27, 2011
Some Day...
I will cough and not start irrationally worrying that it means my cancer has returned, this time in my lungs. That day can't come soon enough.
Monday, May 23, 2011
755 Inches
Wow:

That's the top of Snowbird's home page. They're at 755 inches for the season, which is just shy of 63 feet. I chose a good year to take time off from school. I missed more than a month of skiing after my surgery in November, and then I moved to California at the beginning of March, so I had a shortened season, but even so I got in a 18 days at Snowbird, several of which were truly epic.

That's the top of Snowbird's home page. They're at 755 inches for the season, which is just shy of 63 feet. I chose a good year to take time off from school. I missed more than a month of skiing after my surgery in November, and then I moved to California at the beginning of March, so I had a shortened season, but even so I got in a 18 days at Snowbird, several of which were truly epic.
Sunday, April 17, 2011
My Article in the Yale Daily News
I argue for the importance of making cancer a research a priority before you actually encounter the disease yourself. Of course, it took being diagnosed with cancer for me to realize the importance of this. You can find the article here.
Friday, April 15, 2011
Interesting Status That's Been Floating Around Facebook
A few of my friends have posted this as their status on Facebook:
I'm touched by the sentiment it expresses. I have an objection, though, to its claim that a cancer patient only has one dream. The scariest thing about cancer isn't that it might kill me. What terrifies me the most is that my melanoma might keep me from achieving some of my dreams. So kicking cancer's ass isn't my only dream. Instead, it's the dream that I can only truly achieve through pursuing all my other dreams. That's why I made a point of climbing the tallest mountain I could find before I had Matt take this picture. Climbing mountains is my way of continuing to pursue the dreams that were threatened by my diagnosis.
We have a thousand wishes: To be thinner, be bigger, have more money, a day off, a new phone, to date the person of your dreams. A cancer patient only has one wish: to kick cancer's ass. I know that 97% of you won't post this as your status, but my friends will be the 3% that do. In honor of someone who died, is fighting cancer, or had cancer, post this for at least one hour.
I'm touched by the sentiment it expresses. I have an objection, though, to its claim that a cancer patient only has one dream. The scariest thing about cancer isn't that it might kill me. What terrifies me the most is that my melanoma might keep me from achieving some of my dreams. So kicking cancer's ass isn't my only dream. Instead, it's the dream that I can only truly achieve through pursuing all my other dreams. That's why I made a point of climbing the tallest mountain I could find before I had Matt take this picture. Climbing mountains is my way of continuing to pursue the dreams that were threatened by my diagnosis.
Tuesday, April 5, 2011
FDA Approval for Ipilimumab!
The big news in the world of melanoma this month- or more realistically, this decade- is the FDA's approval of ipilimumab as the first drug ever to show significant benefits for metastatic melanoma patients:
Truly fantastic news!
Incidentally, this article is the first real history of ipilimumab that I've seen. It's pretty dry, but it gives a good sense of how long it took the drug to go from basic research at UC Berkeley 15 years ago to a life saving treatment today.
The U.S. Food and Drug Administration approved a new drug from Bristol-Myers Squibb Co. (BMY) to treat patients with metastatic or late-stage melanoma, the most deadly type of skin cancer.
The drug, ipilimumab, will be sold under the brand name Yervoy. Some analysts have predicted the product will eventually reach blockbuster status with sales topping $1 billion annually. The drug was approved for patients who have tried prior therapy as well as previously untreated patients--a wider patient population than originally expected.
"Late-stage melanoma is devastating, with very few treatment options for patients, none of which previously prolonged a patient's life," said Richard Pazdur, the director of the FDA's office of oncology drug products. "Yervoy is the first therapy approved by the FDA to clearly demonstrate that patients with metastatic melanoma live longer by taking this treatment."
Truly fantastic news!
Incidentally, this article is the first real history of ipilimumab that I've seen. It's pretty dry, but it gives a good sense of how long it took the drug to go from basic research at UC Berkeley 15 years ago to a life saving treatment today.
Saturday, January 29, 2011
Another Couple of Tidbits About Ipi
From an article published last June:
I wrote about the first part of this a couple posts back. The last couple sentences are news to me. It's actually not relevant to my case, since I have been cancer free for quite a while now and don't have any lesions, but it's still interesting.
In related news, it's now been 10 months since I was first diagnosed.
Edit: turns out I first linked to that article on November 2.
Monoclonal antibody treatment also shows several peculiarities. Unlike standard chemotherapy, side effects are a good sign, because they correlate with a strong antitumor response. And progressive disease may not always be a sign of treatment failure: Instead of stalling or shrinking, lesions may actually grow or increase in number during the course of ultimately successful treatment with ipilimumab. This unpredictability has led immunotherapy researchers to develop and adopt a system of immune-related response criteria, an alternative to the WHO's partial/complete response criteria for response to anticancer treatments.
I wrote about the first part of this a couple posts back. The last couple sentences are news to me. It's actually not relevant to my case, since I have been cancer free for quite a while now and don't have any lesions, but it's still interesting.
In related news, it's now been 10 months since I was first diagnosed.
Edit: turns out I first linked to that article on November 2.
Tuesday, January 25, 2011
Post Secret
I read postsecret.com from time to time. Every so often, I'll see a couple that resonate with me. This week, there were two that I can relate to in a way that I couldn't have this time last year. First, there's this:

Two people in particular come to mind when I see this, but I can think of about ten others who it could also apply to. I have the most wonderful people in my life.
I have mixed feelings about the other one:
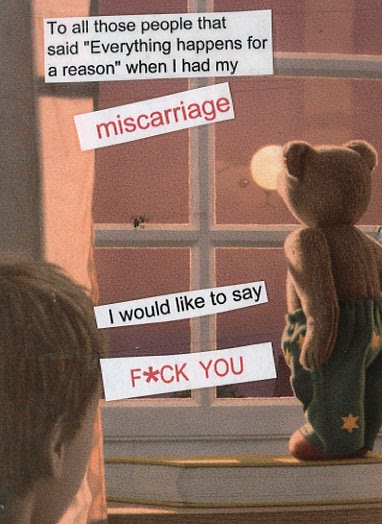
I can't imagine trying to fight cancer without at least hoping that there's some reason that I've been put through hell. But sometimes having someone else assert that there's a reason for it can be quite frustrating. Enough said.
Two people in particular come to mind when I see this, but I can think of about ten others who it could also apply to. I have the most wonderful people in my life.
I have mixed feelings about the other one:
I can't imagine trying to fight cancer without at least hoping that there's some reason that I've been put through hell. But sometimes having someone else assert that there's a reason for it can be quite frustrating. Enough said.
Friday, January 14, 2011
Ipilimumab: Let's not get ahead of ourselves
I read an interesting article today entitled "Ipilimumab for Advanced Melanoma: Let’s Not Throw Caution to the Winds." It's a bit technical, but it makes some good if obvious points.
First, there's only one Phase III trial showing benefits for using ipilimumab in patents with metastatic melanoma, so it's still possible that later trials will show less benefit, particularly in light of that first trial's unconventional design. (The control group was given an experimental vaccine, so if somehow that vaccine actually had a negative effect on survival, that could exaggerate the beneficial effects of ipi.) The authors provide the example of a drug called tremelimumab that (like ipi) targets CLTA-4 and showed some early promise but subsequently failed to show a significiant advantage in Phase III testing. Ipilimumab has more evidence backing its efficacy than tremelimumab ever did, but it is still very much an experimental treatment and later trials may have less positive results.
The other thing is that the side effects of ipilimumab can be very serious. In general, ipi isn't as toxic as chemotherapy, but it can still have side effects like colitis, hypophysitis, hepatitis, and a variety of other autoimmune conditions. In some patients (~1-5%) these side effects can be fatal. I've dealt with some moderate side effects myself, and there's a very real cost associated with that.
Despite lingering questions about its efficacy, ipilimumab still represents a tremendous advance. When I was first diagnosed with melanoma on March 29 of last year, no drug had ever showed an overall survival advantage in a Phase III study for patients with metastatic melanoma. That changed less than a month before my melanoma recurred when the initial paper showing the benefits of ipilimumab on June 5. I really can't get over how lucky I am to live when I do. It's awesome to be part of a trial that (hopefully) will provide more evidence for the efficacy of this drug.
I picked up one piece of information from the article that was pretty exciting to me. Apparently the drug seems to have more success in patients who have significant side effects. I've suspected that this is the case all along, and I'm glad that there's actually evidence to support that conclusion. It definitely makes sense. The drug's only direct effect (as far as I know) is to stimulate the immune system, so the cancer fighting effects and any side effects are going to be a function of how effectively it does that. Consequently, the extent of ipilimumab's side effects are a proxy for how much of an effect the ipi will have on the patient's cancer. I already knew that my side effects meant I'm on the drug rather than the placebo; it's good to know that they also mean the drug is working.
First, there's only one Phase III trial showing benefits for using ipilimumab in patents with metastatic melanoma, so it's still possible that later trials will show less benefit, particularly in light of that first trial's unconventional design. (The control group was given an experimental vaccine, so if somehow that vaccine actually had a negative effect on survival, that could exaggerate the beneficial effects of ipi.) The authors provide the example of a drug called tremelimumab that (like ipi) targets CLTA-4 and showed some early promise but subsequently failed to show a significiant advantage in Phase III testing. Ipilimumab has more evidence backing its efficacy than tremelimumab ever did, but it is still very much an experimental treatment and later trials may have less positive results.
The other thing is that the side effects of ipilimumab can be very serious. In general, ipi isn't as toxic as chemotherapy, but it can still have side effects like colitis, hypophysitis, hepatitis, and a variety of other autoimmune conditions. In some patients (~1-5%) these side effects can be fatal. I've dealt with some moderate side effects myself, and there's a very real cost associated with that.
Despite lingering questions about its efficacy, ipilimumab still represents a tremendous advance. When I was first diagnosed with melanoma on March 29 of last year, no drug had ever showed an overall survival advantage in a Phase III study for patients with metastatic melanoma. That changed less than a month before my melanoma recurred when the initial paper showing the benefits of ipilimumab on June 5. I really can't get over how lucky I am to live when I do. It's awesome to be part of a trial that (hopefully) will provide more evidence for the efficacy of this drug.
I picked up one piece of information from the article that was pretty exciting to me. Apparently the drug seems to have more success in patients who have significant side effects. I've suspected that this is the case all along, and I'm glad that there's actually evidence to support that conclusion. It definitely makes sense. The drug's only direct effect (as far as I know) is to stimulate the immune system, so the cancer fighting effects and any side effects are going to be a function of how effectively it does that. Consequently, the extent of ipilimumab's side effects are a proxy for how much of an effect the ipi will have on the patient's cancer. I already knew that my side effects meant I'm on the drug rather than the placebo; it's good to know that they also mean the drug is working.
Subscribe to:
Comments (Atom)